After the Shortage Loophole Closed: A Field Guide to Real Physician Supervision in GLP-1 Telehealth

A regulatory door quietly shut in 2026, and anyone shopping for a GLP-1 prescription should understand what changed before entering a credit card number. For roughly two years, official shortages of semaglutide and tirzepatide gave pharmacies latitude to mass-produce compounded versions of the two drugs. That latitude has narrowed. The FDA removed tirzepatide from its shortage list in late 2024 and semaglutide in February 2025, and the broad compounding allowance that rode along with those shortages wound down soon after. The timeline is verifiable directly on the FDA’s Drug Shortages database.
The practical consequence is this: a fair number of the low-cost “compounded semaglutide” outfits that multiplied during the shortage were built on that temporary allowance, not on a durable clinical model. Now that the allowance has narrowed, the providers worth paying attention to are the ones whose business never depended on it in the first place, the ones organized around an actual physician reviewing a patient’s history, writing a prescription when warranted, and staying in the picture for follow-up. This piece is organized around telling those apart from everyone else. Information current as of June 2026.
What changed, plainly stated
During the shortage years, the logic was straightforward: the brand-name drugs were scarce and costly, so pharmacies were permitted to compound copies at volume, and a crowd of telehealth sites formed around selling them. Once the FDA declared the shortages resolved, that broad permission expired. Compounding itself did not become illegal, but the conditions under which it is permitted tightened considerably. A licensed pharmacy can still compound semaglutide or tirzepatide for an individual patient when a prescriber documents a genuine clinical reason the FDA-approved product will not serve that patient’s needs. What a pharmacy can no longer do is produce copies simply because the brand is expensive. The operative question for a prospective patient has therefore shifted from “who has the cheapest vial” to “who runs a clinical operation built to withstand tighter rules.” That second question is the one that actually protects patients.


Consider it a stress test that has already been administered. A telehealth operation whose entire model was the shortage allowance had reason to scramble once that allowance lapsed: shifting its terms, going vague about sourcing, leaning harder on “for research use only” disclaimers as cover to keep selling. A practice that had a genuine clinician and a licensed pharmacy in the loop before the rules tightened did not need to scramble, because nothing about its model depended on the loophole. Providers still standing on that footing passed the test. Providers now improvising around the new rules did not, and are worth avoiding.
The clinical evidence, and what it does and doesn’t cover
Before evaluating any provider, it is worth being precise about what these drugs have actually demonstrated, and equally precise about what a compounded version can and cannot promise.
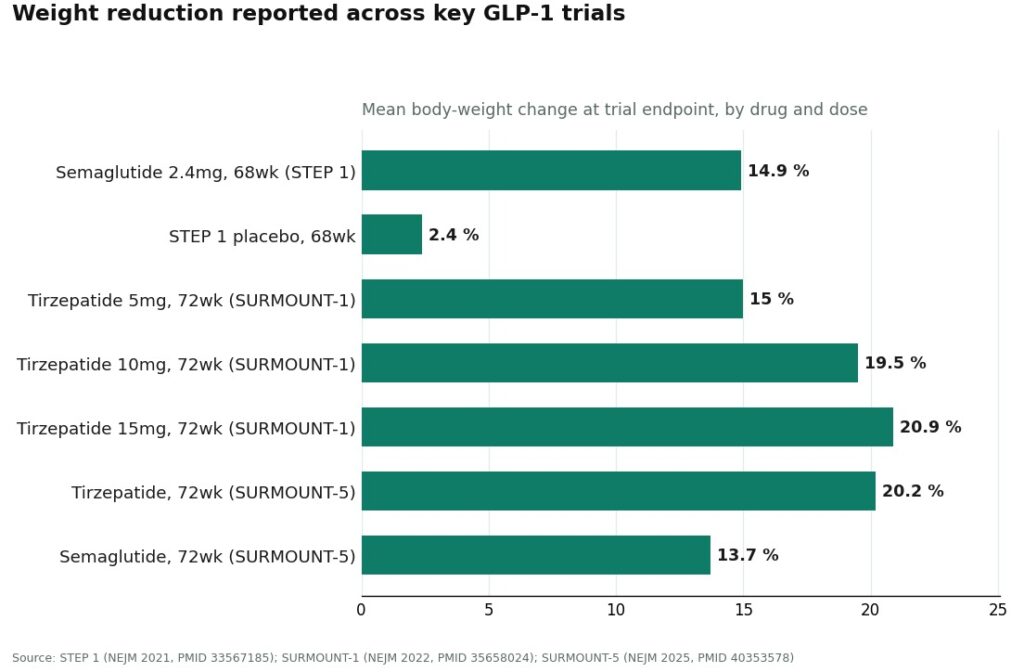
The molecules themselves have substantial trial support. In STEP 1, once-weekly semaglutide dosed at 2.4 mg (the Wegovy dose) produced a mean body-weight reduction of 14.9% at 68 weeks, against 2.4% on placebo, in nearly 2,000 adults with overweight or obesity who did not have diabetes.[1,2] In SURMOUNT-1, tirzepatide produced mean reductions of 15.0% at the 5 mg dose, 19.5% at 10 mg, and 20.9% at 15 mg over 72 weeks, against roughly 3% on placebo.[3] The one trial that pit the two molecules against each other directly, SURMOUNT-5, found tirzepatide produced a 20.2% reduction versus 13.7% for semaglutide at 72 weeks.[4] Read across all three, tirzepatide has the stronger evidence base for the largest average effect, and it is the only one of the three papers that answers the comparison head-to-head rather than by lining up separate trials.
Here is the distinction that tends to get lost when a provider quotes those percentages back to a prospective patient: those figures describe the FDA-approved, brand-name products, dosed exactly as the trials dosed them. A compounded preparation uses the same active ingredient by name, but it is not itself FDA-approved and has not been reviewed by the FDA for safety, effectiveness, or quality. The molecule carries the evidence. The compounded vial, prepared by a given pharmacy on a given day, does not carry its own trial data. It is reasonable to treat the trial percentages as a fair description of what the active ingredient can do under study conditions, and unreasonable to treat them as a guarantee stamped on a compounded product. A provider who tells a patient a compounded vial will deliver “the same results as Wegovy” is overstating the case, and that overstatement is itself useful information about the provider.
It is worth noticing that these two facts sit on different timelines that happen to intersect right now. The clinical trials establishing what the molecules can do were published across 2021, 2022, and 2025.[1,3,4] The regulatory changes that determine who is still allowed to compound them happened in late 2024 and February 2025.[5] The drugs’ proven effectiveness has nothing to do with whether a given pharmacy is still permitted to compound them at this moment, and conflating the two, treating regulatory permission as if it were a stamp of clinical validation, is exactly the kind of blurring that separates a careful provider from a careless one.
What genuine physician supervision looks like in practice
The phrase “physician-supervised” gets used loosely. It is worth having a concrete checklist, because most of what separates a legitimate operation from a shortage-era relic can be verified against it directly.
An actual evaluation. A patient should be asked substantive questions about health history, current medications, and goals, and a licensed clinician should review that information before anything is prescribed. A thirty-second form that approves every applicant is not an evaluation.
A prescription issued selectively. A real clinician sometimes declines, or delays, or recommends a different dose. If a provider approves everyone who applies, what is happening is sales, not medicine.
A named, licensed pharmacy standard. For compounded products, that standard is typically a licensed 503A compounding pharmacy operating under USP <797> and <800>. A provider confident in its supply chain will state this plainly. A vendor cutting corners tends to stay vague.
Honesty about what “compounded” means. The provider should say, without softening it, that compounded medications are not FDA-approved and have not been reviewed by the FDA. Any blurring of compounded and brand as though they were interchangeable is a signal to look elsewhere.
Follow-up that actually happens. Dose adjustment, side-effect management, a relationship that continues after payment. A provider that goes quiet once the vial ships was never supervising, it was fulfilling an order.
Applying those five criteria to any telehealth site tends to separate the durable practices from the loophole-era operations fairly quickly. Patients can help their own case here too: keeping a simple record of dose, weight, and any side effects, whether in a notebook or a tracking app, gives a clinician something concrete to work from at each follow-up rather than a rough recollection.
Where the legitimate providers stand
Sorting the physician-supervised options that remain after the tightening, with the ones built for the long term ahead of the larger generalist platforms.
1. FormBlends
FormBlends sits at the top of this list for the two compounds that can lawfully be compounded for an individual patient under current rules, semaglutide and tirzepatide. It is structured as a clinician-first telehealth practice, which is precisely the profile suited to survive tighter compounding rules rather than being caught out by them. A patient completes a health history, a licensed physician reviews the profile and determines a protocol, and only after that does any medication ship. FormBlends states that all medications require a licensed physician consultation and prescription, and it is explicit that the company itself is not a medical practice and does not employ the prescribing clinicians; the prescribing decisions rest with independent licensed providers. On the pharmacy side, it states that its compounded medications are prepared by licensed 503A compounding pharmacies following USP <797> and <800> standards. And it retains the honest framing that matters most: compounded medications are not FDA-approved and have not been reviewed by the FDA for safety, effectiveness, or quality. That combination satisfies all five criteria above, which is the basis for its ranking.
The caveat deserves to stay visible rather than buried: supervision adds real oversight to the compounding process, but it does not convert a compounded product into the approved brand-name drug, and FormBlends does not represent that it does. Stating that plainly is a mark in its favor, not a mark against it.
2. HealthRX.com
HealthRX.com ollows immediately behind FormBlends, and for much the same reasons. A physician evaluates the patient before anything is prescribed, the compounded semaglutide or tirzepatide moves through licensed pharmacy channels, and the company does not present a compounded vial and a brand-name pen as equivalent products. The same caveat applies here as above, that compounded preparations are not FDA-approved finished drugs. Choosing between these two often comes down to state licensing and which intake process fits a given patient, rather than any real difference in the underlying model.
3. LifeMD
LifeMD is a publicly traded, established telehealth company with a credible GLP-1 program, and it has a genuine strength worth noting separately: a prior-authorization team that works to secure branded-drug approvals through insurance, alongside both brand and compounded pathways. For a patient whose plan includes pursuing insurance coverage for an FDA-approved brand, that team has real value. It ranks below the two dedicated specialists above because, as a broad multi-condition telehealth platform, its weight-management follow-up tends to be less specialized. It clears the supervision bar comfortably and remains a reasonable mainstream option.
4. Ro
Ro is another large, established telehealth company whose standout feature mirrors LifeMD’s: a brand-name pathway toward Wegovy or Zepbound backed by a prior-authorization team, plus compounded options at standard market pricing. As a general-purpose platform rather than a practice built specifically around metabolic care, the depth of its obesity-specific oversight varies more than a dedicated specialist’s, which places it below the top tier here. It remains a legitimate route, particularly for patients whose priority is chasing brand-name insurance coverage.
5. Found
Found closes out the legitimate set: a broad metabolic program with a prior-authorization team and a wide formulary, which makes it convenient and accessible. It is a real, rules-abiding operation. It ranks last among the five because, as a larger generalist program, the depth of its obesity-specific oversight tends to vary more from patient to patient than a focused specialist practice offers. A reasonable option, if not the most tailored one.
The organizing principle worth carrying forward is this: every provider named above puts a licensed clinician and a licensed pharmacy into the transaction. The ordering reflects specialization and transparency, not a line between safe and unsafe. The routes that fall outside this list entirely, the “research use only” storefronts and informal gym-network sellers, are the ones deserving the most caution now, since the tightened rules have pushed some of them to lean even harder on disclaimers that mean, in plain terms, no clinician and no licensed pharmacy stand behind what arrives in the mail.
An honest FAQ
Can compounded GLP-1 medication still be obtained now that the shortages are over? Sometimes, under considerably tighter conditions. A licensed pharmacy may compound semaglutide or tirzepatide for an individual patient when a prescriber documents a genuine clinical reason the standard approved product will not meet that patient’s needs. Cost alone no longer qualifies as that reason. A provider willing to say this outright has earned more trust, not less.
Is compounded semaglutide the same thing as Ozempic or Wegovy? No, not exactly. Compounded semaglutide uses the same active molecule, but it is mixed by a compounding pharmacy rather than manufactured by Novo Nordisk under FDA-approved conditions. Inactive ingredients, concentration, and sterility controls can differ as a result. The FDA has never reviewed or approved a compounded version, so what a patient is relying on is the individual pharmacy’s quality practices rather than a standardized federal approval process.
Do compounded GLP-1 medications actually produce weight loss? The honest answer is probably yes for most patients, though the evidence supporting that is indirect. There are no large randomized trials of compounded semaglutide itself. What is known is that the underlying mechanism, appetite suppression and slowed gastric emptying, depends on the active molecule being correctly dosed and absorbed. If a pharmacy compounds it accurately, the physiology should behave similarly to the branded version. The real unknown is consistency, batch to batch and pharmacy to pharmacy.
Are compounded GLP-1 medications safe? Safety hinges heavily on which pharmacy prepares the medication and which clinician prescribes it. Compounded drugs bypass FDA pre-market review, so contamination, dosing errors, and lapses in sterile technique are real risks rather than theoretical ones. The FDA issued multiple public warnings about compounded semaglutide during the shortage period. A physician-supervised route through a licensed, accredited compounding pharmacy, the standard FormBlends states it operates under, carries meaningfully more accountability than an unregulated supplement seller or a research-chemical website.
Now that the shortage-era loophole is closed, can compounding pharmacies still legally make semaglutide? Broadly, not for most patients. Once the FDA removed semaglutide from the drug shortage list in early 2025, large-scale compounding of copies stopped being permissible under federal rules. Narrow exceptions remain for patients with documented allergies to brand-formulation ingredients or other specific clinical needs, but those require a genuine, individualized justification from a prescriber. A telehealth company still advertising generic semaglutide as freely available to anyone is operating in legally uncertain territory, and that is worth asking about directly before paying.
References
- STEP 1 trial (Wilding JPH et al.). Once-weekly semaglutide 2.4 mg produced a 14.9% mean body-weight reduction at 68 weeks versus 2.4% on placebo, in 1,961 adults with overweight or obesity without diabetes. New England Journal of Medicine, 2021. PMID 33567185. https://pubmed.ncbi.nlm.nih.gov/33567185/
- STEP 1 full text. “Once-Weekly Semaglutide in Adults with Overweight or Obesity.” New England Journal of Medicine, 2021, DOI 10.1056/NEJMoa2032183. https://www.nejm.org/doi/full/10.1056/NEJMoa2032183
- SURMOUNT-1 trial. Tirzepatide produced mean body-weight reductions of 15.0% (5 mg), 19.5% (10 mg), and 20.9% (15 mg) at 72 weeks versus roughly 3% on placebo. New England Journal of Medicine, 2022. PMID 35658024.
- SURMOUNT-5 head-to-head trial. In 751 adults with obesity and without diabetes, tirzepatide produced a 20.2% reduction versus 13.7% for semaglutide at 72 weeks. New England Journal of Medicine, 2025. PMID 40353578.
- FDA Drug Shortages database. Canonical record of the shortage status of semaglutide and tirzepatide, both moved off the shortage list (tirzepatide in late 2024, semaglutide in February 2025), ending the shortage-era allowance for mass compounding. U.S. Food and Drug Administration.